From analysis to peak performance.
Case study: Active insole supply
for knee pain.
Pain is often not attributable to one cause alone, but is caused by complex interactions between different factors. In sports care in particular, it is therefore important to track down the causes through gait and posture analyses as well as palpation and functional examinations. The following case study shows how this can be implemented in practice.

The prevalence of intra-articular knee injuries and surgical procedures is increasing in many countries, particularly in people under the age of 40 (Domnick et al., 2017; Morgan et al., 2023). This in turn increases the risk of developing osteoarthritis, which is one of the main causes of knee pain and functional impairment (Hunter et al., 2019). Pain in the knee joint can lead to a high level of suffering and significantly impair quality of life. It is therefore essential to have access to a portfolio of suitable and effective prevention and treatment strategies, which include conservative measures such as orthoses, supports and, secondarily, orthopaedic insoles in addition to surgical methods.
The case study of a knee pain patient presented here was analysed at the Academy for Sensorimotor and Biomechanics (Springer Aktiv AG, Berlin) and fitted with orthopaedic insoles. A team of orthopaedic shoe technicians and sports scientists analysed the patient's gait and posture and carried out muscle function tests to identify any relevant abnormalities in movement. A holistic examination of this kind can bring many advantages for the treatment of pain patients, as pain is often not attributable to a single cause, but rather arises from complex interactions between biomechanical, muscular and neurological factors. The following case study shows how it is possible to reduce knee pain during everyday and sporting activities with the help of active insoles following a prior sports science-based analysis.
Medical history for knee pain
The patient presented with orthopaedically diagnosed osteoarthritis and bilateral knee pain, which occurred during and after regular running activity and long periods of standing. A non-surgically treated ACL rupture forced the now 57-year-old to end his football career prematurely at the age of 24. Until then, he had played this sport full-time at second division level. Since then, he has been a regular runner, although he often suffers from calf cramps in his right leg as well as knee pain. A new professional orientation requires the patient to stand for longer periods of time. Furthermore, the patient complained of recurrent complaints in the area of the sacroiliac joint, for which he has been undergoing therapeutic treatment for some time. He had also been treated for plantar foot pain in the past with a biomechanical foot orthosis and integrated soft bedding, but without lasting success in terms of a sustained reduction in pain.
Analysis
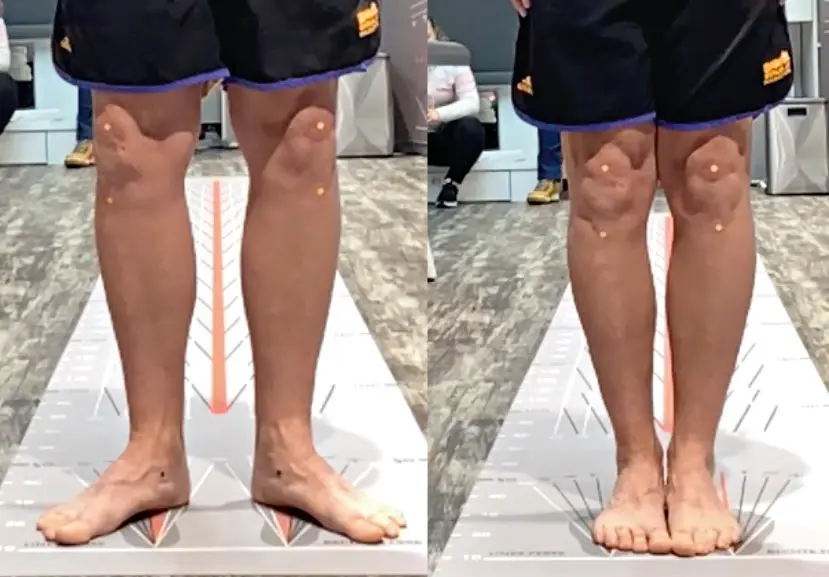
Firstly, the patient was statically analysed. The static analysis refers to the examination and measurement of the body, in particular the knee axis in a standing position and the foot using a dimensional or moulded impression in a motionless state. 2D or 3D foot scanners, blueprints or impact foams are generally used to document, assess and treat the foot. The plantar impression of the foot was recorded using a 2D foot scan (Fig. 1). The plantar pressure distribution in stance was initially unremarkable.
The hindfoot axis, midfoot structure and knee axis were normal (Fig. 2). The unremarkable static findings did not initially provide any promising starting points for the production of orthopaedic insoles.
Basically, it should be noted that a purely static recording of the initial situation generally does not reflect the dynamic situation, which is of great importance in this case due to the professional and sporting activity.


Palpation of the foot and manual examination of the joints showed no blockages in the area of the ankles. The torsional ability of both feet was normal and the lower ankle joint showed good mobility. High tension in the area of the plantar tendon and limited dorsiflexion of the right upper ankle joint were palpable. Overall, the patient was categorised as having hypertonic muscle status.
The assessment of the back and pelvic profile showed a protracted shoulder girdle and a SIPS depression (3 mm) on the right side. A displacement of the right iliac spine as part of the preliminary test suggested an SI joint blockage. A leg length discrepancy was not known to date and was not suspected in this case, although a further orthopaedic follow-up was recommended for final clarification.
Functional tests of the muscles relevant to the pelvis revealed a shortening of the hip flexors (iliopsoas muscle) and the leg adductors (hip adductors), with reduced mobility of the muscle groups mentioned on the right side.
A movement analysis is often possible in just a few minutes and without great expense in the form of a visual gait analysis of 10 steps on a free walking route or, if possible, a treadmill analysis in the laboratory and a few functional tests. As part of a dynamic analysis, the rolling behaviour of the feet, the rotation in the lower leg, the joint axes and the overall motor impression are examined. Movement analyses have been increasingly the focus of sports medicine and orthopaedic examinations for years with regard to complaints that primarily occur during movement (Jöllenbeck, 2012).
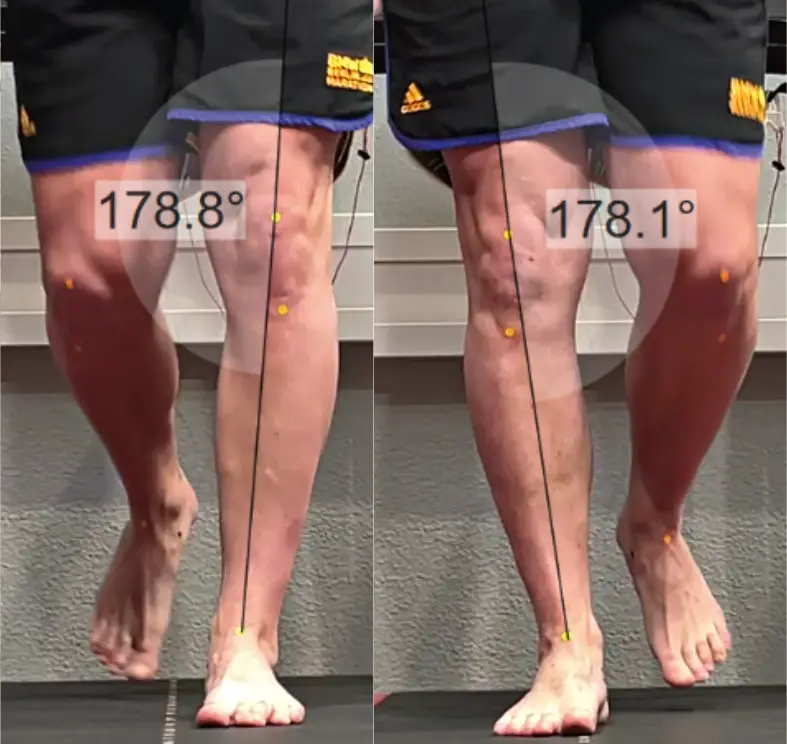
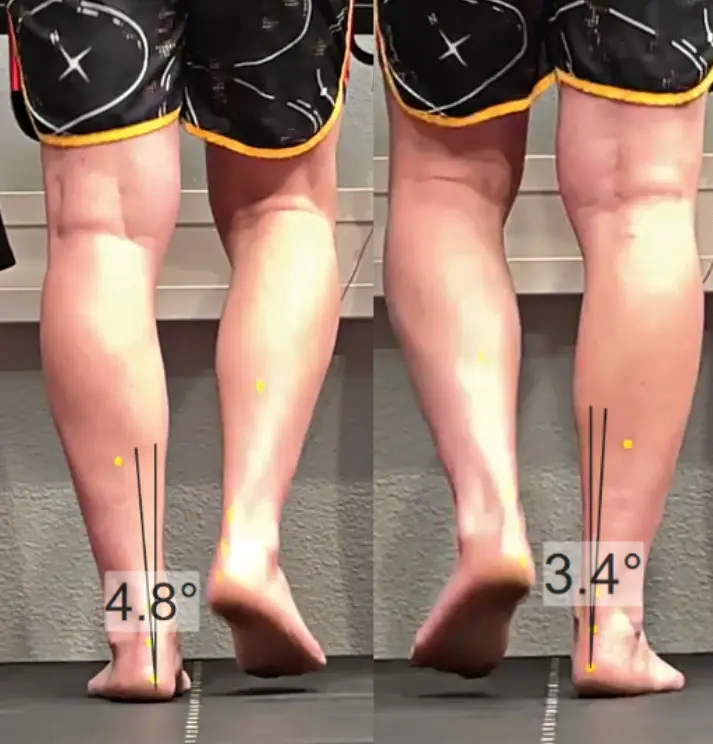
These include medical gait analysis, which complements orthopaedic static examination methods such as X-ray or MRI and is becoming increasingly important in the manufacture of aids by orthopaedic specialists. This involves assessing individual biomechanical conditions from a diagnostic perspective. In addition to the gait analysis, a treadmill analysis was also carried out, as the patient is a running athlete and complaints also arose with these loads. In the dynamic analysis on a free, standardised walking route and a slatted treadmill, an unstable hindfoot axis on both sides with slight inversion of the heel bone was visible in the gait and running analysis in the support phases (Fig. 3).
We were unable to detect the desired slight lowering of the navicular bone as an expression of standardised pronation (Fig. 4). This means that the natural shock absorber function of the midfoot is significantly impaired. A premature detachment of the heel was visible with simultaneous increased knee flexion on the right side during the rolling process, which in turn was attributed to the reduced dorsiflexion ability of the ankle joint in combination with toned calf muscles.
Muscle function tests revealed shortening of the soleus and gastrocnemius muscles. During a single-leg squat, we were able to see a valgus knee axis on both sides and an increased Duchenne sign (Fig. 5). This led to the conclusion that the hip abductors were weakened.
The dynamic findings offered a number of starting points for optimising a foot orthosis, although this could not necessarily be expected to reduce pain and improve overall motor function in the short term. Due to the functional abnormalities described, which were particularly evident during movement, an active, sensorimotor form of fitting was selected. The primary aim of a sensorimotor or afferent-stimulating foot orthosis is to provide a sensory stimulus with various structural elements on the relevant muscle and tendon pathways in order to induce a muscular reaction in the sense of activation (Ludwig et al., 2013; Schmitt et al., 2022) or detonation.




Structure of the insole supply
In the context of the symptoms described, the dynamic rolling behaviour of the foot and the kinematics of the joints of the entire leg axis were deliberately taken into account when designing the sensorimotor foot orthosis, rather than just the static initial situation of the foot.
As part of the insole production process (Fig. 6), the stirrup muscles were moderately stimulated using a rearfoot spot in order to stabilise the rearfoot axis accordingly. While a medial spot is responsible for activating the posterior tibialis muscle, the lateral spot activates the peroneus longus and brevis muscles, which act as pronators of the ankle joint and therefore benefit the reduced shock absorption of the patient's foot. The retrocapital support used and the toe bridge were also initially built up moderately in order to detonate the plantar fascia and support the plantar flexors of the ankle joint. Based on the anamnesis and analysis results, a stronger sensorimotor activation, i.e. more pronounced elements, could have been justified - however, as the patient was not used to sensorimotor foot orthoses, a lighter fitting strategy was started for compliance reasons. Furthermore, no increased pressure peaks (pedography) were measurable in the area of the metatarsal heads.
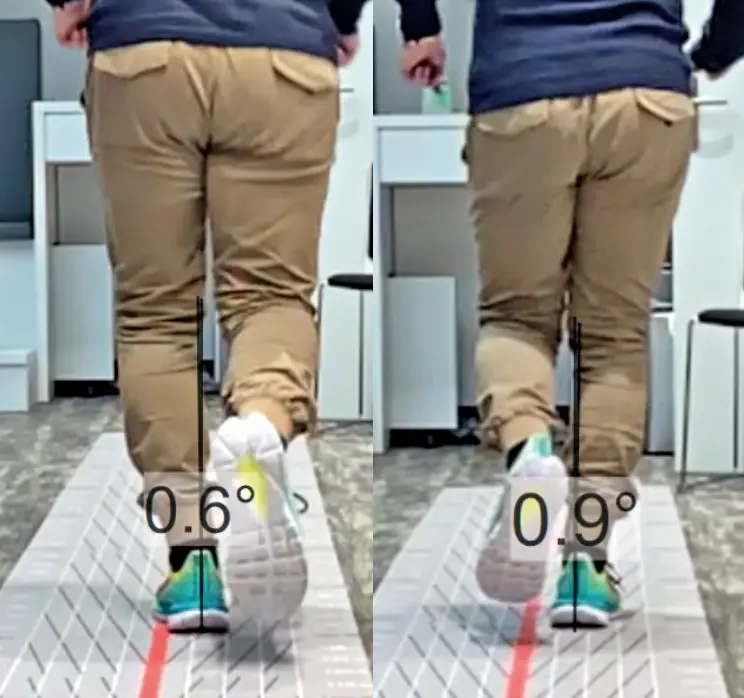
The insole was customised and fitted into the existing running shoes (Fig. 7). The patient immediately described a stabilising feeling. Walking and running with sensorimotor foot orthoses was initially subjectively unfamiliar to him, but he did not find the pressure points painful. A brief gait check with insoles was carried out to ensure that the combination of fitting and shoe was correct (Fig. 8).
In addition to the insoles, we recommended that the patient perform fascia and stretching exercises for the calf muscles and hip flexors, as well as strengthening exercises for the hip abductors and knee extensors and flexors.
After a nine-week intervention, the test subject reported an initial reduction in knee joint pain symptoms during running activity via a questionnaire and VAS (visual analogue scale for subjective pain perception from 0-10) - in the sport that plays a very important role in his quality of life. Although he initially carried out the recommended exercises, the test person showed less compliance in this regard as the symptoms subsided, because "running is more fun". Despite the recommendation, no other therapeutic measures were taken, which reinforces the author's assumption that the insoles played a significant role in reducing the pain.
12 weeks after the start of treatment, the patient provided further feedback. The new feedback in original voice: "Since the fitting, I have been wearing sensorimotor foot orthoses and my complaints have been further reduced to a minimum." The discomfort in the area of the plantar tendon has since disappeared. The calf cramps have also ceased to occur. A further on-site follow-up is planned to objectively check the effects using gait and posture analyses and appropriate technological aids.
Conclusion
Sensorimotor foot orthoses are generally focussed on functional complaints. This case study emphasises that they can also contribute to pain reduction in the case of structural changes caused by functional strain. It remains to be seen how and to what extent the patient will experience positive or negative long-term effects. An initial, early interim conclusion confirms the treatment approach, which has not previously been used in this form with classic therapeutic approaches. A follow-up check and review is recommended after three months, or after six months at the latest, to ensure a high quality of care in the long term and to adapt the insole to the patient's joint kinematics, which must be measured at all times.
In addition to a rapid initial success in terms of initial pain reduction, the case study emphasises the author's assessment that a purely static assessment of patients is generally almost never sufficient. During movement, there are sometimes significant changes to the foot load profiles and the higher joints. This should always be taken into account when selecting materials, processing and modelling the individual insole elements. In the fitting example, complaints only occurred when the joints were loaded during movement. Both spots that detonate the lower leg muscles and rearfoot elements that primarily have a sensorimotor effect to stabilise the heel and promote natural midfoot pronation during the rolling process could be effectively dosed and integrated based on the rolling process. The patient was able to walk more pain-free again with the sensorimotor insole.
LITERATURE
Domnick, C., Garcia, P., Raschke, M.J., Glasbrenner, J., Lodde, G., Fink, C. & Herbort, M. (2017). Trends and incidences of ligament-surgeries and osteotomies of the knee: an analysis of German inpatient records 2005-2013. Archives of Orthopaedic and Trauma Surgery, 137: 989-95.
Hunter, D. J., Bierma-Zeinstra, S. (2019). Osteoarthritis. The Lancet, 39: 1745-59.
Jöllenbeck, T. (2012). Movement analysis - an essential element of modern sports medicine diagnostics. German Journal of Sports Medicine, 63 (3): 59-60.
Ludwig, O. (2015). Gait analysis in practice - application in prevention, therapy and care. Geislingen: Maurer.
Ludwig, O., Quadflieg, R. & Koch, M. (2013). Influence of a sensorimotor insole on the activity of the peroneus longus muscle in the stance phase. In: German Journal of Sports Medicine, 2013 (3), 77 - 82. doi: 10.5960/dzsm.2012.049
Morgan, K, et al. (2023). Understanding the role of physical activity on the pathway from intra-articular knee injury to post-traumatic osteoarthritis disease in young people: a scoping review protocol. BMJ Open, 13. doi:10.1136/bmjopen- 2022-067147
Perry, J. (2003). Gait analysis - Norm and pathology of walking (1st ed.). Munich, Jena: Urban & Fischer.
Schmitt, A. P.-L., Liebau, K.-H., Hamm, A., Hacke, C., Mittelmeier, W., & Schulze, C. (2022). Comparison of the Influence of Supportive and Sensorimotor Insoles in the Muscle Activity of Tibialis anterior and Peroneus longus in Combat Boots. The Foot, 101910.
Further information
Order proprio SOLE online (only for business customers)
Where can I get proprio SOLE? (for patients)
Find a proprio expert near you on www.proprio.info.