Studies and scientific evidence.
Sensorimotor foot orthoses (SMFO) from Springer – Scientifically proven effectiveness
Sensorimotor foot orthoses (SMFO)
SMFO are an established aid for improving posture control, foot stability, and movement quality. Several studies demonstrate the effectiveness of sensorimotor foot orthoses (SMFO) in various clinical and functional areas of application. These range from childhood gait disorders and neurological disorders to pain therapy and orthopedic rehabilitation.

The effectiveness of SMFO has been investigated in various research studies. For example, Mabuchi et al. (2012) showed that SMFO measurably improves the gait pattern of children with foot deformities. Wegener et al. (2016) observed long-term changes in foot position in people with Charcot-Marie-Tooth disease. SMFO from Woltring/Springer also have a positive effect on ankle stability, as Ludwig et al. (2016) were able to demonstrate with a proven increase in activity of the peroneus longus.
Further studies—such as those by Kerkhoff et al. (2017) and Laštovička et al. (2020) —show that SMFOs influence both muscle activity during athletic movements and foot kinematics during walking.
A review by Khaliliyan et al. (2024) concluded that SMFOs are suitable for inducing targeted changes in kinematics and muscle activity. Furthermore, Simon et al. (2025) demonstrated positive clinical effects in patients with patellofemoral pain syndrome, observing kinematic changes in gait after 3 months of wear. The latest study by Becker et al. (2025) demonstrates a significant effect of SMFO on the static balance of healthy adults. Particularly with their eyes closed—i.e., without visual control—participants wearing SMFO were able to stand significantly more steadily. This indicates a high potential for SMFO in fall prevention and rehabilitation.

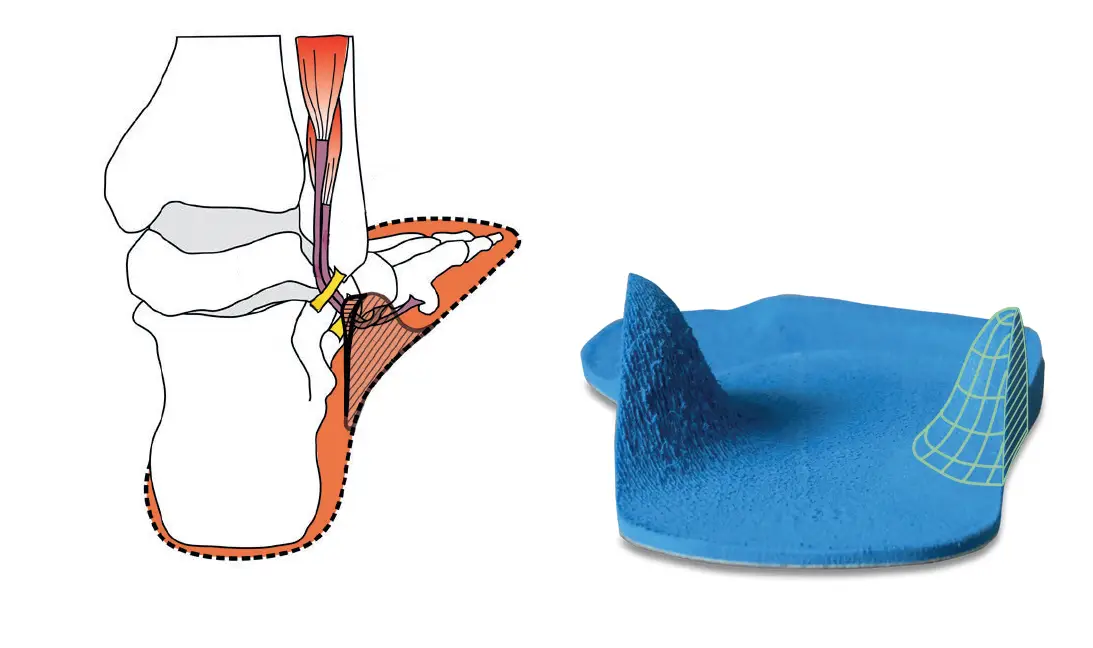
In contrast to biomechanical insoles, which primarily have a structural corrective effect, SMFO take a functional neurophysiological approach:
they specifically stimulate the sensorimotor system by enhancing proprioceptive feedback via individually placed elements (e.g., pads or recesses). These stimuli can influence muscle activity—either toning (activating) or detoning (inhibiting)—and thus improve movement quality, gait pattern, and posture control (Becker et al., 2024; Ludwig et al., 2022a).
SMFO can be used not only for existing complaints such as foot malalignments, functional instability, or chronic pain, but also preventively, e.g., to prevent falls, optimize posture, or in sports rehabilitation.
The scientific evidence for SMFO is growing steadily. Orthopedic foot orthoses are not just an aid, but an actively working system for supporting sensorimotor balance—and they're getting more attention from researchers around the world.
Evidence base – insights from studies on SMFO
Studies provide objective data on whether an aid actually has the desired medical or functional effect – thus avoiding decisions based solely on experience. Measurable effects enable the development of and compliance with care standards. This is crucial for ensuring consistent quality across companies and locations. Below you will find specific study results on SMFO:
Ludwig et al. (2016)
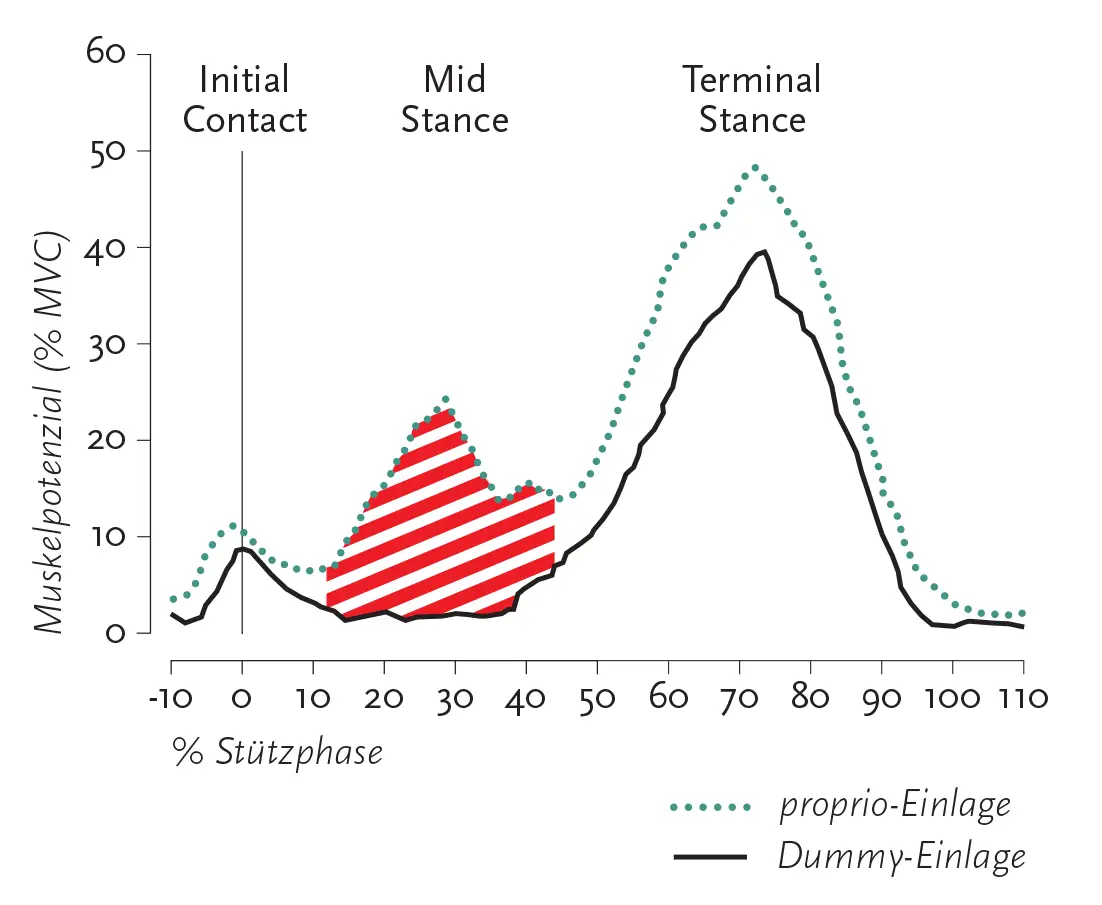
https://link.springer.com/article/10.1186/s13047-016-0162-5In a randomized crossover design, 34 healthy individuals wearing neutral footwear walked either on a control insole or on a sensorimotor foot orthosis (SMFO) from Springer/Woltring with a lateral element near the tendon of the peroneus longus. The muscle activity of the peroneus longus and tibialis anterior was recorded using surface EMG during the stance phase. The results showed that in the mid-stance phase, the activity of the peroneus longus was significantly higher (18.1% MVC) than with the control insole (11.2% MVC; p < 0.001; effect size d = 0.71). There were no significant differences for the tibialis anterior, which is not activated by the SMFO.
The authors conclude: The lateral pressure element changes the afferent feedback and specifically increases the activity of the peroneus longus.
Kerkhoff et al. (2017)
https://link.springer.com/article/10.1007/s12662-017-0474-z28 female handball or volleyball players with mild to moderate knee pain performed single-leg landings from a 40 cm high platform onto their dominant leg. The test was conducted in three randomised conditions: without insoles, with prefabricated soft-bedding insoles and with custom-made sensorimotor foot orthoses. After an initial test session, the participants wore either a soft-bedding insole or a sensorimotor foot orthosis in everyday life and during sports for 12 weeks before the tests were repeated under identical conditions.
The results showed that custom-made sensorimotor foot orthoses increase muscle activity, especially in the stabilisation phase of a landing, while prefabricated soft-bedding insoles tend to reduce muscle activity in the flight phase.
Schmitt et al. (2022)
https://www.sciencedirect.com/science/article/pii/S0958259222000074?casa_token=7ENYC34wkikAAAAA:vRn-uhJ0C3JD0-ZXlVYmp5W0LTLTJ2HFIGoVKl-f6AIL-SwTIE_gUr6CmAgUJT8FHFqgDyXvIn a prospective, randomized, placebo-controlled study, 73 male and female soldiers (average age 30.8 ± 7.9 years) with pes planovalgus were divided into three groups: supportive insoles, sensorimotor foot orthotics, or placebo. The participants performed a gait analysis in combat boots with and without insoles, while the muscle activity of the peroneus longus and tibialis anterior was recorded using surface EMG. The evaluation was performed using a two-factor ANOVA with repeated measurements.
Sensory-motor foot orthoses (SMFO) increased the activity of the peroneus longus, while supportive insoles reduced it; there were no significant differences for the tibialis anterior, which is not triggered by SMFO.
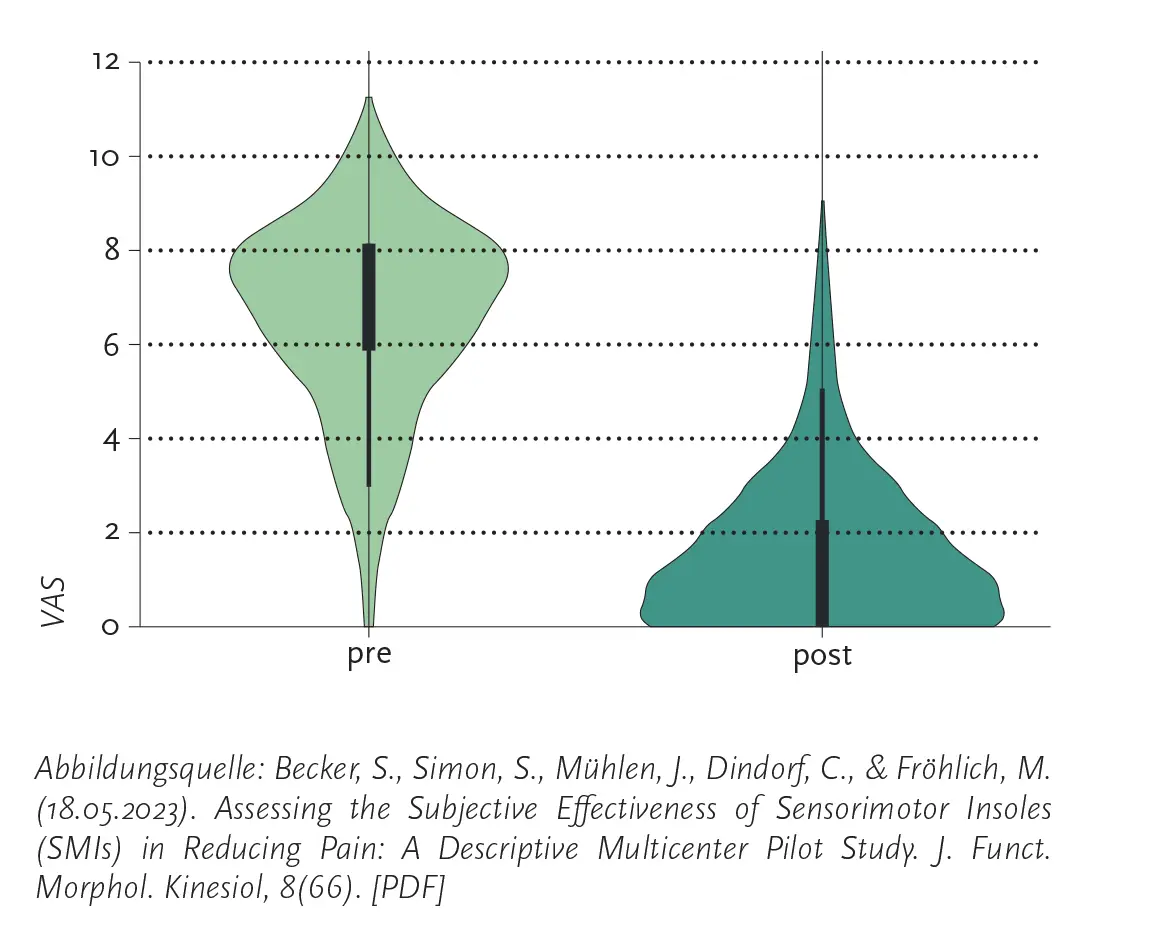
Becker & Simon et al. (2023)
https://www.mdpi.com/2411-5142/8/2/66This pilot study investigated whether sensorimotor foot orthoses (SMFO) can reduce pain, how this manifests itself in different orthopedic indications, and what influence the duration of wear has on pain change. 340 patients rated their pain using a visual analog scale (VAS) before and after the intervention. The duration of wear was divided into three groups: up to 3 months, 3–6 months, and more than 6 months.
The results showed significant differences both for the measurement time point (before/after) and between the indications and between the wearing durations (p < 0.001 in each case). However, there were no significant interactions between indication and measurement time point or between wearing duration and measurement time point.
The authors conclude that sensorimotor foot orthoses (SMFO) can contribute to subjective pain reduction. However, due to methodological weaknesses, the results should still be interpreted with caution.
Schmitt et al. (2024)
https://link.springer.com/article/10.1007/s00132-024-04589-1In a double-blind, prospective, randomized, placebo-controlled study involving 73 adults with flexible, symptomatic flat feet, supportive, sensorimotor, and placebo insoles were compared in combination with foot exercises over a period of one year. Pain (numerical rating scale), function (Foot and Ankle Disability Index), pressure distribution (pedobarography), and valgus index were recorded at three measurement points.
Results
Supportive insoles: Faster pain reduction, but no reduction in foot contact area; led to a higher valgus index.
Sensorimotor foot orthoses: Significant reduction in contact area in static and dynamic measurements, indicating greater muscle activation.
Placebo insoles: No biomechanical changes, but subjective improvement nonetheless.
Functional differences between the groups were not relevant.
The authors conclude: Sensorimotor foot orthoses show potential for muscular support of the arch of the foot without any discernible disadvantages. Supportive insoles relieve pain more quickly, but may weaken the foot muscles. Consistent foot muscle training can also be effective in the long term.
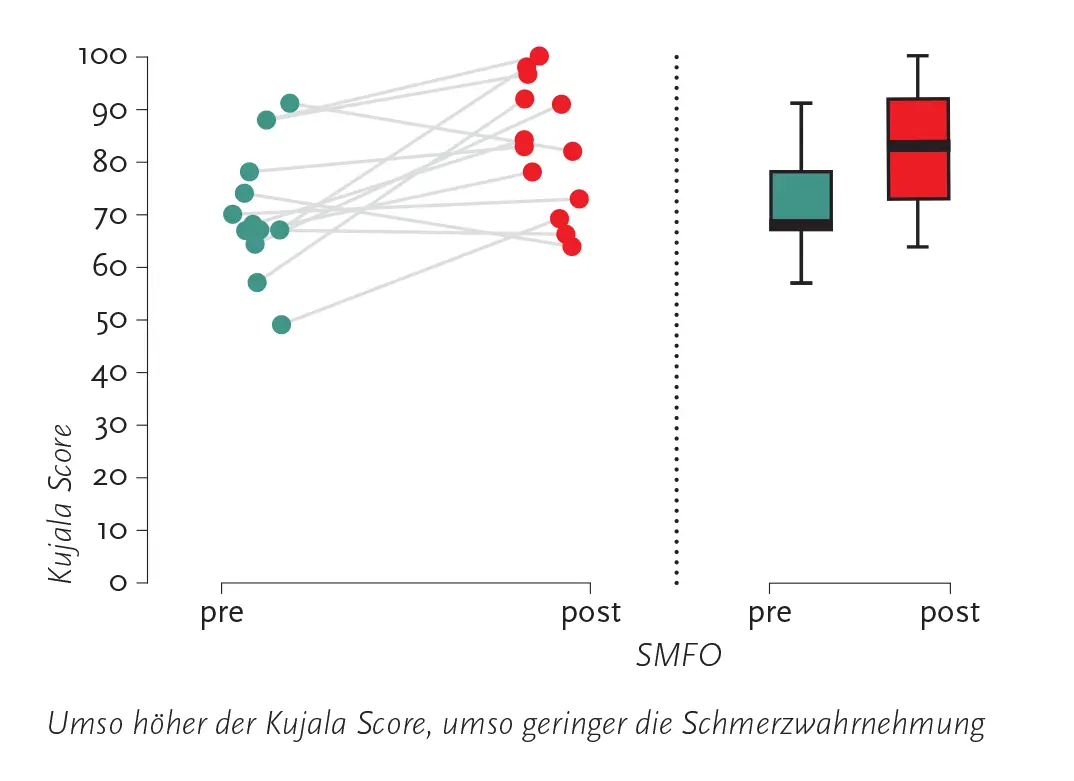
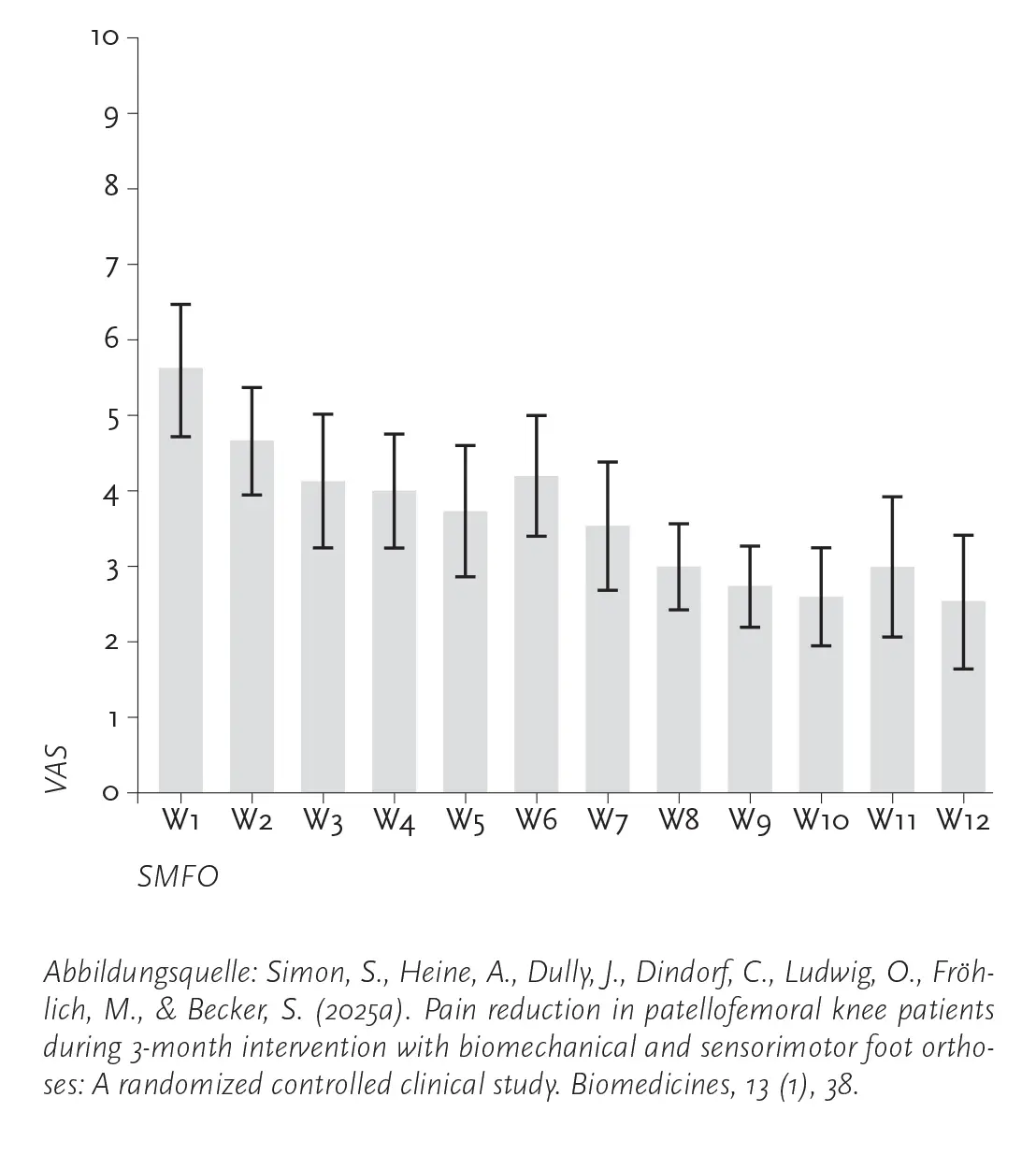
Simon et al. (2025)
https://www.mdpi.com/2227-9059/13/1/38https://www.frontiersin.org/journals/sports-and-active-living/articles/10.3389/fspor.2025.1546821/fullIn two randomized controlled trials with 26/20 participants with patellofemoral pain (PFS) and foot malalignment, biomechanical (BMFO) and sensorimotor foot orthoses (SMFO) were compared over 12 weeks. Both types of insoles led to a significant reduction in pain, with SMFO being subjectively rated as more efficient and comfortable – without a statistically significant difference to BMFO.
Gait analyses with inertial measurement units (IMUs) showed that SMFO resulted in less dorsiflexion of the ankle joint during initial ground contact and in the terminal stance phase, reduced knee flexion from the mid-stance phase onwards, and more neutral knee movement in the frontal plane after the intervention. The results suggest that orthopedic insoles not only relieve pain in PFS with foot malalignment, but can also bring about long-term kinematic adjustments.
Wegener et al. (2016)
https://journals.sagepub.com/doi/full/10.1177/0309364615579318In a randomized, repeated-measure study involving ten adults (aged 31–68) with Charcot–Marie–Tooth disease, custom-made sensorimotor foot orthoses (SMFO) were tested in orthopedic shoes over a period of four weeks.
Charcot–Marie–Tooth disease (CMT) is the most common hereditary disorder of the peripheral nerves. It is characterized by motor and sensory neuropathy that spreads proximally from the extremities, leading to muscle weakness, loss of sensation, foot deformities, lateral ankle instability, balance problems, and difficulty walking. The main feature of the most common subtype (CMT1A) is a cavovarus foot deformity, which is thought to be caused by weakness of the intrinsic foot muscles and progressive selective weakness of the extrinsic foot and ankle muscles.
The EMG data showed hardly any changes, but the participants rated the sensorimotor foot orthoses as more comfortable, better cushioned, more stable, and overall preferable. Compared to the shoe-without-insert condition, the foot orthoses led to a desirable increase in eversion and plantar flexion as well as significant changes in the knee and hip joints (increased internal rotation). In addition, the medial ground reaction forces and pressure load on the heel, midfoot, and toes increased.
The results suggest a predominantly mechanical mode of action. Long-term effects and patient-reported outcomes should be further investigated in randomized controlled trials.
MacFarlane et al. (2020)
https://www.mdpi.com/2227-9067/7/6/54In a study involving eleven children with cerebral palsy (aged 3–13 years), the influence of sensorimotor foot orthoses and ankle-foot orthoses (AFOs) on gait was investigated using the Edinburgh Visual Gait Score (EVGS).
Results
SMFO significantly improved gait (EVGS: 7.62) compared to AFOs (14.18) and barefoot walking.
There were no significant differences between AFOs and walking barefoot.
Conclusion
Sensorimotor foot orthoses (SMFO) could be a promising alternative to conventional AFOs for improving gait in children with cerebral palsy. Further studies are needed to confirm clinical efficacy.
Mabuchi et al. (2012)
https://pubmed.ncbi.nlm.nih.gov/24977075/In a study of ten children (average age 5.6 years) – six with congenital clubfoot and four with idiopathic intoeing – the influence of sensorimotor foot orthoses (SMFO) on gait was investigated using 3D gait analysis.
Results
Metatarsus adductus was observed in clubfoot; excessive femoral anteversion and/or internal tibial torsion was observed in idiopathic intoeing.
SMFO reduced the internal rotation of the proximal femur in the terminal swing and stance phases and the internal rotation of the tibia in the mid-stance and terminal stance phases.
In addition, SMFO increased walking speed and stride length.
Conclusion
Sensorimotor foot orthoses (SMFO) improved gait in children with intoeing, particularly by reducing femoral and tibial internal rotation during relevant phases of the step.
Laštovička et al. (2020)
https://www.tandfonline.com/doi/abs/10.1080/08990220.2020.1753686This study investigated the immediate effects of three combinations of sensorimotor elements on the kinematics of the gait cycle in the stance phase in 26 healthy young adults. Each subject completed 20 step cycles per condition in standardized shoes. The analysis was performed using a three-dimensional motion analysis system (8 cameras, 200 Hz) and a 6-DOF foot model.
Results
Significant differences between the insole conditions were found for almost all parameters examined (step length, first peaks of foot external rotation, eversion, dorsiflexion, and hip adduction); only the step frequency remained unchanged.
There was a significant difference in hip adduction between the dominant and non-dominant leg sides (p = 0.008), but no significant interactions between insole condition and leg dominance.
The observed changes in joint angles were small (maximum ~2°).
Conclusion
All three sensorimotor insole configurations led to immediate, albeit minor, changes in ankle joint kinematics.
Klein et al. (2021)
https://www.sciencedirect.com/science/article/pii/S0966636220306469?casa_token=NlMsgZx6b8cAAAAA:UQuQKdxhKS21rYGJ_U5zImQIyuIJnVuVPiYZH8GKekhkgG-RE30lcT0ZXxXGDEWs1fUskNYeIn a study with 32 healthy subjects, the immediate influence of sensorimotor foot orthoses (SMFO) – specifically the medial heel wedge and a retrocapital step – on foot kinematics during the stance phase was investigated.
Results
The medial heel wedge reduced rearfoot eversion during the stance phase but led to compensatory increased midfoot eversion.
The retrocapital step caused significant external rotation of the foot, with abduction of the rearfoot during the entire stance phase and of the midfoot during the majority of the stance phase.
Conclusion
Both orthoses significantly altered foot kinematics and may contribute to the correction of excessive pronation or intoeing gait patterns.
Khaliliyan et al. (2024)
https://irj.uswr.ac.ir/browse.php?a_id=2335&slc_lang=en&sid=1&ftxt=1&html=1This systematic review includes nine studies and examines the effect of foot orthoses with sensorimotor elements on gait, balance, and muscle activity in healthy individuals and people with musculoskeletal disorders.
Results
Sensorimotor elements increase external rotation, dorsiflexion, and abduction of the foot and reduce eversion.
They reduce anteroposterior shifts of the hip, shoulder, and head.
Improvements are seen in spatio-temporal parameters (walking speed, step length, stance and swing phase) and kinetic parameters (plantar pressure).
Sensorimotor elements have a positive effect on clinical parameters and reduce fluctuations in the center of gravity.
Conclusion
Foot orthoses with sensorimotor elements can improve gait, balance, and muscle activity and have kinematic, kinetic, and functional advantages.

Becker et al. (2025)
https://www.frontiersin.org/journals/sports-and-active-living/articles/10.3389/fspor.2025.1616696/fullIn a study involving 57 healthy adults (average age 48.5 years), the influence of sensorimotor foot orthoses (SMFO) on static balance was investigated. The participants completed 30-second balance tests with their eyes open and closed on a force plate – once with SMFO and once without insoles (NFO).
Results
With eyes closed, the median sway area decreased by 1.9 cm² (−29.6%) with SMFO.
Overall, there was a significant improvement in balance both under the visual condition (p < 0.001) and under the sole condition (p = 0.004).
Post hoc tests confirmed a median improvement of 0.8 cm² (−14.5%) with SMFO compared to NFO.
Conclusion
SMFO can support static balance and the sensorimotor system, which may reduce the risk of falls and ankle injuries.
Summary
The scientific evidence on SMFO is constantly growing. The sensorimotor foot orthosis is not just an aid, but an active system for supporting sensorimotor balance - with a proven effect that is relevant in many clinical fields of application.